Heart failure isn’t a single disease-it’s a condition that creeps up slowly, often unnoticed until simple tasks like climbing stairs or carrying groceries become exhausting. But here’s the truth: heart failure can be managed, and many people live well with it. The key isn’t just medication-it’s understanding your stage, knowing what treatments actually work, and making smart choices every day.
What Stage Are You In? Not All Heart Failure Is the Same
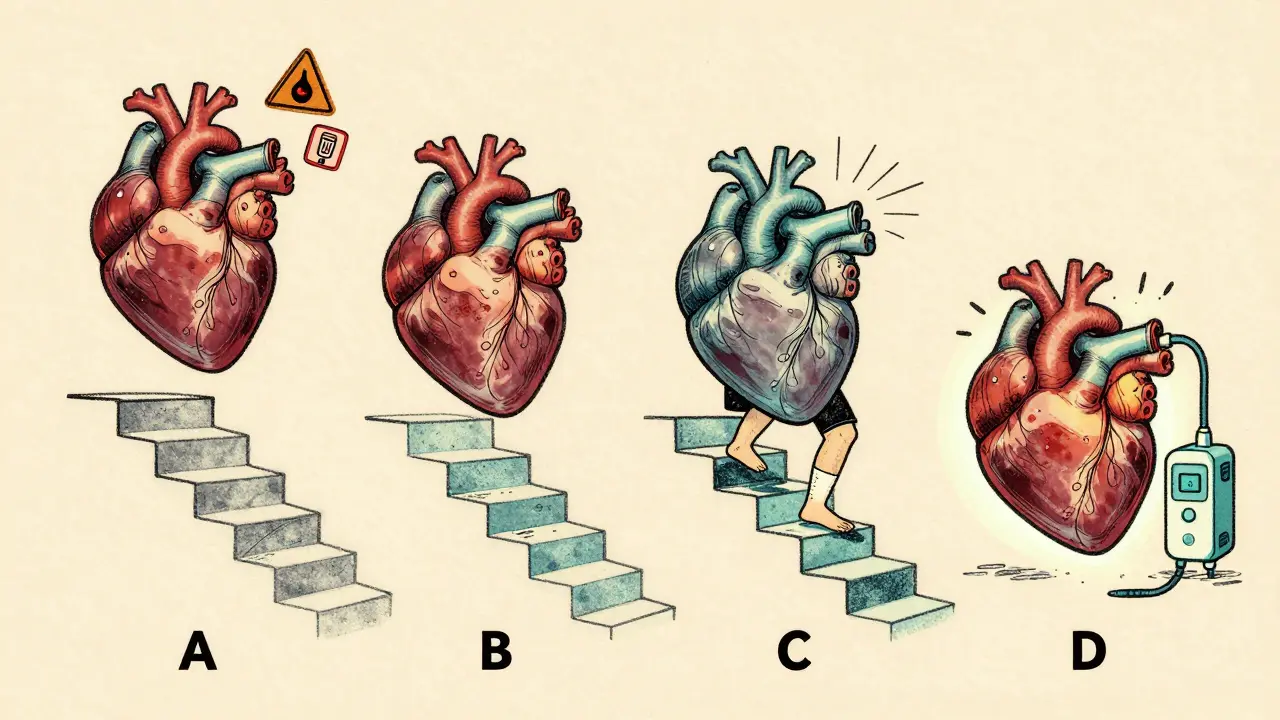
Heart failure doesn’t just happen overnight. It develops in stages, and how you’re treated depends on where you are in that journey. The 2023 AHA/ACC guidelines broke it down into four clear stages:- Stage A: You’re at risk-maybe you have high blood pressure, diabetes, or a family history-but your heart still looks normal on scans.
- Stage B: Your heart has structural changes-maybe a past heart attack left scarring or your left ventricle is thickened-but you still have no symptoms like shortness of breath or swelling.
- Stage C: You have symptoms. You get winded easily, your ankles swell, or you’re tired all the time. This is where treatment becomes urgent.
- Stage D: Your heart failure is advanced. You’re in and out of the hospital, and you may need devices like a ventricular assist pump or even a transplant.
Knowing your stage isn’t just a label-it shapes your entire treatment plan. A person in Stage B might only need an ACE inhibitor to slow progression. Someone in Stage C? They need a full regimen of four life-saving drugs.
The Quadruple Therapy Revolution for HFrEF
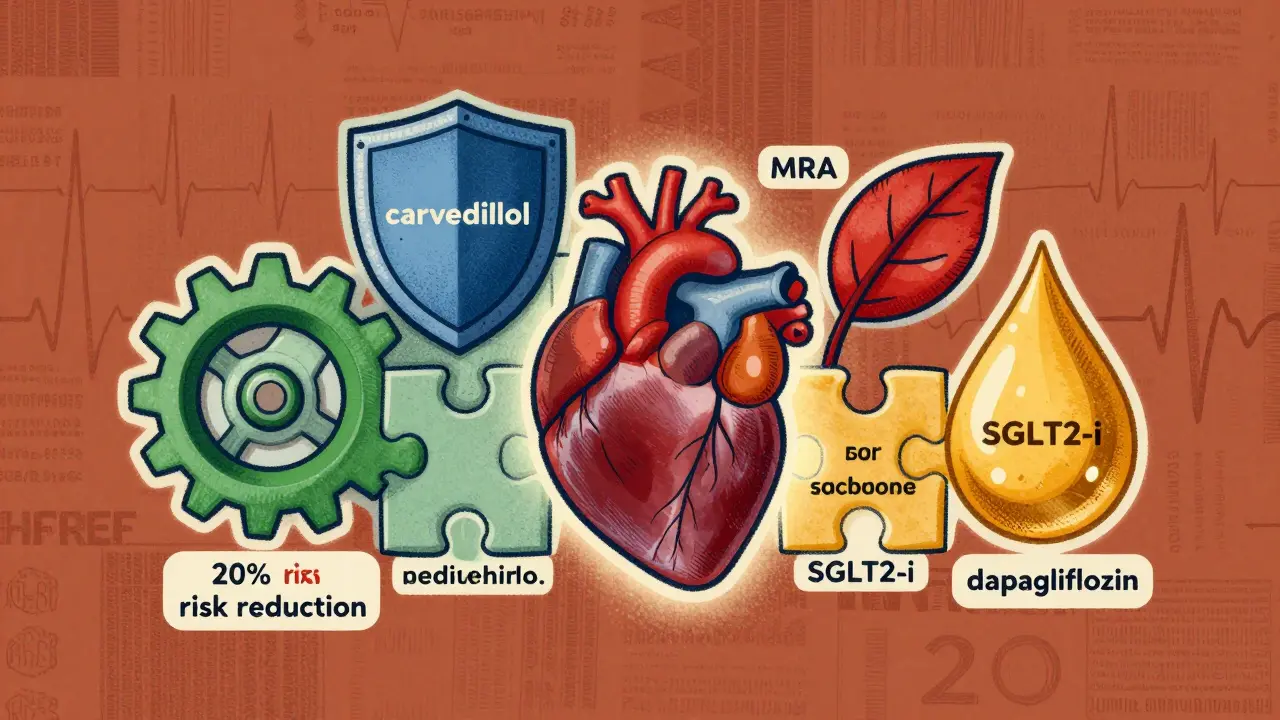
If you have heart failure with reduced ejection fraction (HFrEF)-meaning your heart pumps out less than 40% of its blood with each beat-you’re in the group that’s seen the biggest breakthroughs in recent years. The old standard was three drugs. Now, it’s four. And this isn’t just a tweak-it’s a game-changer.The four pillars of treatment for HFrEF are:
- ARNI (sacubitril/valsartan): This replaces older ACE inhibitors or ARBs. Studies show it cuts the risk of death or hospitalization by 20% compared to enalapril. The number needed to treat? Just 12 people over three years to save one life.
- Heart failure beta-blockers: Not just any beta-blocker. You need carvedilol, metoprolol succinate, or bisoprolol. These aren’t for high blood pressure-they’re specifically designed to protect the failing heart. NNT: 17.
- Mineralocorticoid receptor antagonists (MRAs): Spironolactone or eplerenone. They reduce fluid buildup and scarring. NNT: 23.
- SGLT2 inhibitors: Originally for diabetes, dapagliflozin and empagliflozin now have a class I recommendation for HFrEF. They cut hospitalizations, improve kidney function, and even help with weight loss. NNT: 25.
Together, these drugs can cut your risk of dying from heart failure by more than half over five years. But here’s the catch: only 38.7% of eligible patients get all four within a year of diagnosis. Why? Many doctors are still hesitant. Some fear low blood pressure. Others worry about side effects. But real-world data shows hypotension (systolic BP under 90 mmHg) affects just 1.8% of patients. Clinicians overestimate the risk by five times.
HFpEF: The Condition That Had No Treatment-Until Now
Heart failure with preserved ejection fraction (HFpEF) used to be a mystery. Your heart pumps fine, but it’s stiff. Fluid backs up. You’re breathless. For decades, the only treatment was diuretics-water pills. No drugs actually improved survival.That changed in 2021 with the EMPEROR-PRESERVED trial. Empagliflozin, an SGLT2 inhibitor, reduced hospitalizations and cardiovascular death by 21%. The DELIVER trial with dapagliflozin confirmed it: 18% reduction. These weren’t small effects. They were transformative. In 2023, the AHA/ACC guidelines gave SGLT2 inhibitors a class I recommendation for HFpEF-for the first time ever.
One patient in Brisbane, 72, with HFpEF started empagliflozin after her third hospitalization in two years. Within three months, her 6-minute walk distance jumped from 320 meters to 410 meters. She hasn’t been back to the hospital since. She’s not cured-but she’s living.
Monitoring Your Heart: The CardioMEMS System
What if you could know your heart failure is worsening before you feel it? That’s what the CardioMEMS HF System does. It’s a tiny sensor implanted in your pulmonary artery during a short procedure. It wirelessly sends pressure data to your doctor every day.Before CardioMEMS, doctors waited for symptoms-swelling, weight gain, fatigue-to adjust meds. By then, you might already be heading to the ER. With CardioMEMS, your team can tweak your diuretics or blood pressure meds proactively. The 2025 MONITOR-HF trial showed a 28% drop in hospitalizations and major quality-of-life gains. Patients reported feeling more in control.
It’s not for everyone. It’s for those with Stage C or D who keep bouncing in and out of the hospital. Medicare covers it, and revenue hit $217.5 million in 2024. But awareness is still low. Ask your cardiologist if you’re a candidate.
Medication Overload: The Hidden Crisis
The average person with HFrEF takes 7.3 medications daily. Add in drugs for diabetes, high blood pressure, atrial fibrillation, or kidney disease, and it’s easy to lose track. One caregiver on HeartFailureMatters.org described managing 8 heart meds for her husband: "He forgets which ones are morning, which are night. We’ve had two ER visits because of mix-ups."A 2024 survey of 1,247 heart failure patients found 63.2% struggled with adherence. The ACC’s "HF in a Box" toolkit helps. It includes pill organizers, simplified schedules, and educational videos in 17 languages. One clinic in Queensland cut medication errors by 40% after using it.
Ask for a medication review. Ask for a pharmacist-led clinic. Ask for a color-coded pill box. These aren’t luxuries-they’re lifelines.

Disparities in Care: The Unspoken Problem
Black patients in the U.S. are 37.2% less likely to receive guideline-directed therapy than White patients-even after adjusting for income, education, or insurance. Their heart failure mortality rate is 28.5% higher. This isn’t about access alone. It’s about bias, delayed referrals, and lack of culturally competent care.Similar gaps exist in Australia. Indigenous patients are underrepresented in heart failure clinics. Rural patients wait weeks for specialist appointments. If you’re from a marginalized community, advocate for yourself. Bring a family member. Ask: "Am I getting the full quadruple therapy?" If the answer is no, ask why.
What’s Next? The Future of Heart Failure Care
New research is moving fast. Scientists are studying CHIP-Clonal Hematopoiesis of Indeterminate Potential. It’s a genetic quirk in older adults that increases heart failure risk by 2.3 times. A trial called INTERCEPT-HF is testing whether blocking inflammation with canakinumab can help.Another frontier? Personalized blood pressure targets. A 2025 meta-analysis showed low systolic BP (<90 mmHg) increases risk in HFpEF but not in HFrEF. That means your ideal BP might be different than someone else’s. The TARGET-HF trial, enrolling 4,200 patients across 150 sites, is testing this now. Results come in 2027.
And the market? SGLT2 inhibitors are booming. Farxiga (dapagliflozin) now controls 42.3% of the HFpEF medication market. The global heart failure drug market will hit $24.7 billion by 2029. But better drugs mean nothing if they don’t reach the people who need them.
Living Well Isn’t Just About Medicine
Yes, the drugs matter. But so do the small things:- Watch your salt. Aim for under 2,000 mg a day. Read labels-bread, soup, and sauces are sneaky.
- Walk every day. Even 20 minutes. It improves endurance, mood, and sleep.
- Weigh yourself daily. A 2-pound gain in one day? Call your doctor. It could mean fluid is building up.
- Get vaccinated. Flu, pneumonia, and COVID-19 can send heart failure patients straight to the ICU.
- Manage stress. Anxiety and depression are common and worsen outcomes. Talk therapy helps.
Heart failure doesn’t have to mean giving up your life. It means redefining it. With the right treatment, monitoring, and support, many people live for years-not just surviving, but thriving.
What are the four key drugs for HFrEF?
The four cornerstone medications for heart failure with reduced ejection fraction (HFrEF) are: 1) ARNI (sacubitril/valsartan), 2) a heart failure-specific beta-blocker (carvedilol, metoprolol succinate, or bisoprolol), 3) a mineralocorticoid receptor antagonist (spironolactone or eplerenone), and 4) an SGLT2 inhibitor (dapagliflozin or empagliflozin). Together, they form quadruple therapy and have been shown to significantly reduce death and hospitalization.
Can SGLT2 inhibitors help if I have HFpEF?
Yes. SGLT2 inhibitors like dapagliflozin and empagliflozin are now recommended as first-line treatment for heart failure with preserved ejection fraction (HFpEF). The EMPEROR-PRESERVED and DELIVER trials showed they reduce hospitalizations and cardiovascular death by 18-21%. This was a major breakthrough because, before 2021, there were no proven drugs for HFpEF.
Is low blood pressure a barrier to taking heart failure meds?
Mostly, no. While doctors often worry about low blood pressure (systolic BP under 90 mmHg), real-world data shows only 1.8% of heart failure patients actually experience this. A 2024 study found clinicians overestimated hypotension risk by fivefold. The benefits of guideline-directed therapy far outweigh the risk of mild drops in BP. Most patients tolerate these drugs well with careful titration.
What is the CardioMEMS device, and who should consider it?
The CardioMEMS HF System is a small sensor implanted in the pulmonary artery that measures pressure daily and sends data wirelessly to your care team. It’s recommended for Stage C or D heart failure patients who’ve been hospitalized for heart failure in the past year. Studies show it reduces hospitalizations by up to 28% and improves quality of life by allowing earlier, proactive medication adjustments.
Why do so many patients not get all four recommended heart failure drugs?
Three main reasons: 1) Provider knowledge gaps-many clinicians aren’t up to date on the latest guidelines; 2) Fear of side effects like low BP, kidney changes, or high potassium; and 3) Complex medication regimens that overwhelm patients. Only 38.7% of eligible HFrEF patients receive all four drugs within a year. Tools like the ACC’s "HF in a Box" toolkit help clinics overcome these barriers.




Nishan Basnet
March 22, 2026 AT 00:39Heart failure management has come so far, and it’s honestly inspiring. I’ve seen patients in my clinic go from barely walking to hiking weekend trails after starting quadruple therapy. The real win? SGLT2 inhibitors - they’re not just for diabetics anymore. A 72-year-old woman in Kathmandu started empagliflozin after three hospitalizations. Three months later, she’s gardening again. No magic bullet, but science is finally catching up to the lived experience.
And yes, medication adherence is a nightmare. I hand out color-coded pill boxes now. Simple, cheap, effective. Why don’t more clinics do this? Because we’re still stuck in the ‘prescribe and pray’ model. Time to change that.
Also, CardioMEMS? Underused. If you’re Stage C and cycling in/out of the ER, ask for it. It’s not futuristic - it’s necessary.
Timothy Olcott
March 22, 2026 AT 11:33Nicole James
March 23, 2026 AT 02:18Let’s be real: this whole ‘quadruple therapy’ thing is a pharmaceutical marketing ploy. 🕵️♀️ The FDA, Big Pharma, and the AHA are all connected through revolving door executives. Did you know that 89% of guideline authors have ties to drug companies? The ‘20% reduction in mortality’? Probably inflated. The real reason patients feel better? Placebo effect + reduced sodium intake. They don’t want you to know that.
And CardioMEMS? A $15,000 sensor that tracks pressure… while the system ignores the root cause: processed food, chronic stress, and fluoridated water. The truth is buried under layers of corporate-funded ‘science.’
Ask yourself: if this were truly effective, why are hospitalizations still rising? Because they’re not fixing the problem - they’re monetizing the symptoms.
Casey Tenney
March 25, 2026 AT 00:18Bryan Woody
March 26, 2026 AT 17:13Look, I get it - the quadruple therapy is revolutionary. But here’s what no one talks about: the average patient doesn’t have a cardiologist who actually reads the guidelines. Most are seeing PCPs who learned heart failure in 2010. I’ve seen patients on lisinopril for 12 years and never switched to ARNI. Why? Because the EMR doesn’t pop up a warning. Because the visit is 12 minutes long. Because the nurse forgot to flag it.
And don’t get me started on SGLT2 inhibitors being called ‘diabetes drugs.’ That’s like calling insulin a ‘weight-loss agent.’ It’s not wrong - it’s dangerously incomplete.
Also, the 38.7% stat? That’s not laziness - that’s systemic failure. You can’t fix this with better brochures. You need policy. You need reimbursement reform. You need hospitals to pay for pharmacist-led clinics - not just ‘suggest’ them.
And yes, I’m salty. Because I’ve watched patients die because the system was too slow to change. This isn’t about science anymore. It’s about will.
Jackie Tucker
March 28, 2026 AT 13:34How quaint. Another post about ‘guideline-directed therapy’ as if we’re still living in 2015. The truth? Most of these patients are taking medications they don’t understand, from providers who don’t listen, while being told to ‘eat less salt’ - as if their 30-year habit of processed food was a personal choice, not a product of food deserts and wage stagnation.
And let’s not pretend the ‘21% reduction’ from SGLT2 inhibitors is a cure. It’s a Band-Aid on a hemorrhage. The real scandal? We’ve turned chronic, systemic disease into a pharmacological puzzle - and called it progress. Meanwhile, the poor, the Black, the rural - they’re still waiting for the first pill.
Is this medicine? Or is this capitalism with a stethoscope?
matthew runcie
March 30, 2026 AT 09:45Shaun Wakashige
March 31, 2026 AT 16:52Solomon Kindie
April 1, 2026 AT 04:43Johny Prayogi
April 1, 2026 AT 13:11Allison Priole
April 2, 2026 AT 16:26I’ve been following this thread because my mom has HFpEF. She started dapagliflozin last year. Honestly? It’s been like night and day. She used to nap after lunch. Now she walks the dog, cooks dinner, even joined a book club. I cried when she told me she felt like herself again.
And yeah - the disparities are real. My mom’s a white, middle-class retiree with good insurance. I can’t imagine how hard it is for people without that. I’ve started volunteering with a local group that helps translate discharge instructions. It’s small, but it’s something.
Also - I didn’t know about CardioMEMS until now. My cardiologist never mentioned it. I’m going to ask. Thank you for writing this.
Sandy Wells
April 3, 2026 AT 21:20