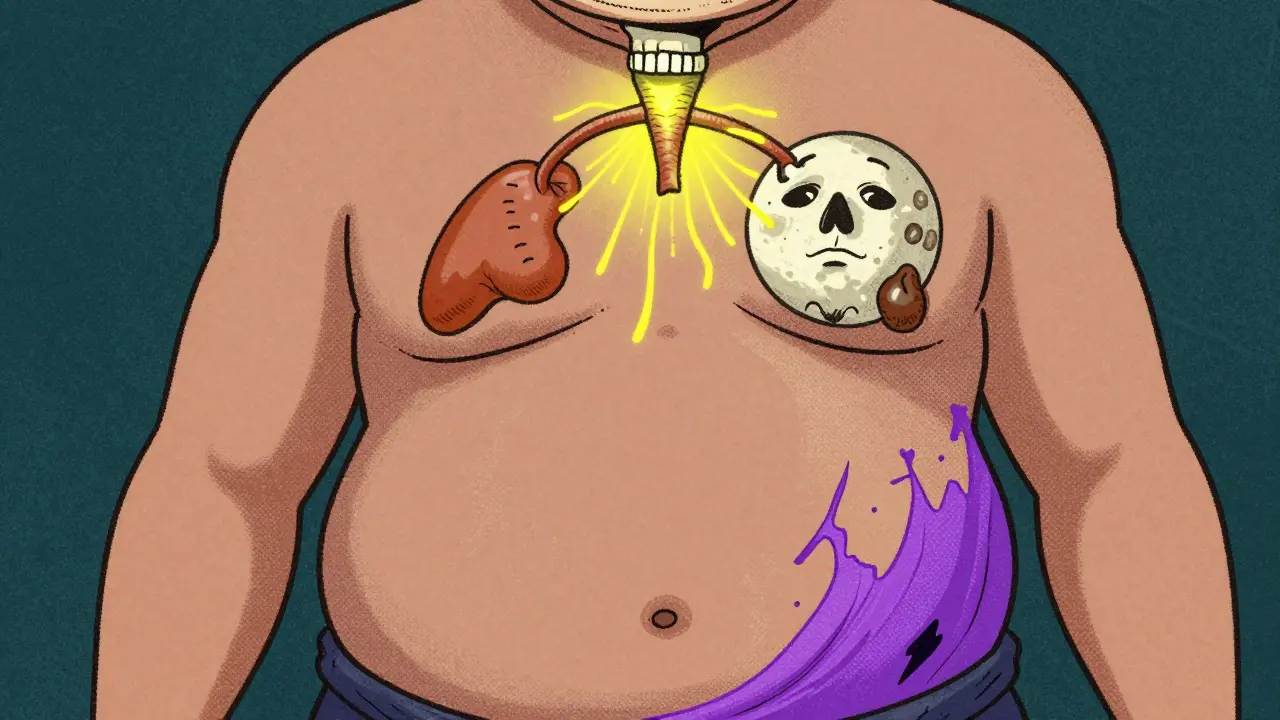
Cushing’s Syndrome isn’t just weight gain or a moon-shaped face-it’s a serious hormonal imbalance that can break down your body if left untreated. When your adrenal glands pump out too much cortisol, your metabolism goes haywire, your bones weaken, your blood pressure spikes, and your immune system starts to fail. This isn’t a case of stress gone wrong. This is your body being flooded with a hormone meant for short-term survival, and it’s stuck in overdrive. For many, the only path to real recovery is surgery.
What Causes Cushing’s Syndrome?
Cushing’s Syndrome happens when your body is exposed to too much cortisol for too long. About 80% of cases come from outside your body-like taking steroid pills for asthma, lupus, or rheumatoid arthritis. But the other 20%? That’s endogenous Cushing’s, where your own body makes too much. This is the kind that needs surgery.Most endogenous cases (60-70%) are caused by a tiny, noncancerous tumor in the pituitary gland. This tumor overproduces ACTH, the signal that tells your adrenal glands to make cortisol. That’s called Cushing’s disease. About 15-20% come from tumors on one adrenal gland itself. And in 5-10% of cases, tumors elsewhere-like in the lungs or pancreas-start pumping out ACTH like a broken faucet. These are harder to find, but they’re treatable.
Here’s what the numbers show: a 24-hour urine cortisol level over 50 mcg is a red flag. Normal is 5-25 mcg. Late-night saliva cortisol above 0.14 mcg/dL? That’s abnormal. And if your cortisol doesn’t drop after a low-dose dexamethasone pill, your body isn’t listening to its own brakes. These aren’t vague symptoms. These are measurable, repeatable signs that point to one thing: your cortisol is out of control.
Physical Signs You Can’t Ignore
You don’t need a lab test to suspect Cushing’s. The physical signs are unmistakable if you know what to look for.Think of it like this: your body’s fat distribution gets rewired. You gain weight around your stomach and face, but your arms and legs stay thin. That’s central obesity-trunk-heavy, limb-light. Your face swells into a round, flushed moon. A fatty hump builds at the base of your neck-a buffalo hump. Purple stretch marks appear on your abdomen, thighs, and breasts. Not the faint silvery ones from pregnancy. These are wide, deep, and vividly violet. They’re not cosmetic. They’re a sign your skin is literally tearing under the pressure of too much cortisol.
Bone density drops fast. Half of all patients develop osteoporosis with a T-score below -2.5. That means even a minor fall can break a hip. Blood pressure climbs above 140/90 in 85% of cases. Blood sugar turns erratic-70% develop prediabetes or full-blown diabetes. Your muscles weaken. You get tired. Your mood swings. You might stop menstruating. Or your immune system gets so suppressed you get infections that won’t heal.
These aren’t random side effects. They’re direct consequences of cortisol’s role in breaking down muscle, storing fat, raising glucose, and suppressing inflammation. When cortisol is too high for too long, your body starts eating itself.
Why Surgery Is the First-Line Treatment
Medication can help manage symptoms. Drugs like pasireotide or mifepristone can block cortisol or reduce its production. But they don’t fix the source. They’re temporary. And they cost $5,000 to $10,000 a year-out-of-pocket for many.Surgery, on the other hand, removes the problem at the root. For pituitary tumors, transsphenoidal surgery-through the nose-is the gold standard. It’s minimally invasive. No scalp incision. No brain retraction. Just a tiny path to the tumor. Success rates? 80-90% for tumors under 10 mm. Even for larger ones, you still have a 50-60% chance of remission. That’s far better than drugs.
For adrenal tumors, a laparoscopic adrenalectomy removes the whole gland. It’s a 1-2 hour procedure. Hospital stay? Usually just one night. Success rate? 95%. And once the tumor’s gone, cortisol levels drop fast. Many patients notice their energy returning within weeks. The moon face fades. The stretch marks lighten. Blood pressure improves.
But here’s the catch: it only works if you go to the right place. A 2023 study in the Journal of Neurosurgery found that surgeons who do fewer than 10 pituitary surgeries a year have remission rates around 50-60%. Those who do 20 or more? 80-90%. Volume matters. Experience matters. A center that sees one Cushing’s case a month won’t give you the same outcome as one that sees five.
What the Surgery Actually Involves
For pituitary tumors: You’re put under general anesthesia. The surgeon slips a thin scope through your nostril, past the sphenoid sinus, and into the base of your skull. Using a microscope or endoscope, they find the tumor-sometimes no bigger than a pea-and remove it. The procedure takes 2-4 hours. You’re usually out of the hospital in 2-5 days.For adrenal tumors: Two or three small incisions in your abdomen. A camera and tools go in. The adrenal gland is detached and removed. It’s quicker-1-2 hours. You’re often home the next day. Both procedures have low complication rates: bleeding, infection, or CSF leak (fluid around the brain) happen in less than 5% of cases.
But there’s one big risk everyone talks about: adrenal insufficiency. After removing the tumor, your body doesn’t know how to make cortisol anymore. For weeks or months, you’ll need replacement steroids-hydrocortisone. About 30-40% of patients need this temporarily. 5-10% need it for life. That’s not a failure. It’s expected. And it’s manageable with proper dosing.
What Happens After Surgery
Recovery isn’t just about healing the incision. It’s about relearning how your body works.For the first 6-12 weeks, you’ll need frequent blood tests to monitor cortisol and ACTH. Your steroid dose will be adjusted slowly. Too much? You’ll gain weight again. Too little? You could go into adrenal crisis-low blood pressure, vomiting, shock. That’s why patients are taught to give themselves extra steroids during illness, injury, or stress. A simple cold could be dangerous if you don’t.
Most patients feel better within 3-6 months. One patient on a Cushing’s support forum wrote: “Two months after surgery, my moon face vanished. My blood pressure went from 160/100 to 110/70 without meds. I lost 40 pounds.” That’s not rare. Studies show 72% of patients report major symptom improvement within six months.
But not everyone recovers fully. About 28% deal with lingering fatigue, hormone deficiencies, or emotional struggles. Some need thyroid or testosterone replacement. A few need a second surgery. And 10-25% of pituitary cases come back over 10 years. That’s why follow-up is lifelong. Quarterly endocrine visits. Annual bone scans. Regular blood pressure checks.
The Real Cost of Delaying Surgery
Waiting to treat Cushing’s isn’t just risky-it’s expensive in ways you can’t measure.A 2021 study from the Mayo Clinic showed that patients who waited more than two years after diagnosis had 30% lower remission rates after surgery. Why? Because prolonged high cortisol damages your heart, your bones, your kidneys. Your risk of heart attack, stroke, or infection climbs. Even after successful surgery, your mortality rate stays 1.5 to 2 times higher than the general population.
And it’s not just physical. The emotional toll is heavy. Many patients describe losing years of their lives-unable to work, exercise, or even leave the house. One Reddit user, diagnosed at 34, said: “I couldn’t hold a job. My marriage fell apart. I felt like a ghost in my own body.”
Surgery isn’t just about removing a tumor. It’s about reclaiming your life. The earlier you act, the better your odds.
What to Look for in a Surgical Center
Not all hospitals are created equal when it comes to Cushing’s.The Endocrine Society recommends centers that perform at least 20 pituitary surgeries per year. These places have teams-endocrinologists, neurosurgeons, nurses, radiologists-all trained in Cushing’s. They know how to interpret tricky imaging. They know how to handle post-op steroid management. They know the signs of recurrence.
Look for centers with dedicated Cushing’s programs. Ask: How many pituitary surgeries do you do a year? What’s your remission rate? Do you have a nurse coordinator for post-op care? Do you use intraoperative cortisol monitoring? New devices approved by the FDA in 2023 can tell surgeons within 24 hours if the tumor’s fully removed-cutting hospital stays by two days.
If you’re in the U.S., check if the center is part of the NIH-funded CUREnet registry. These sites follow standardized protocols and report outcomes publicly. That’s accountability.
Is Surgery Right for You?
If you’ve been diagnosed with endogenous Cushing’s and have a confirmed tumor, surgery is your best shot at cure. Medications are a bridge-not a destination.But surgery isn’t for everyone. If you have other serious health problems-uncontrolled diabetes, heart failure, severe lung disease-you may need to stabilize those first. Surgery under those conditions increases complication risk by 300%.
And if your tumor can’t be located? Or if it’s too risky to remove? Then medical management becomes the plan. But even then, surgery remains the goal. It’s the only treatment that can fully restore your natural hormone balance.
For most, the choice isn’t whether to have surgery. It’s when. The clock is ticking. Every month of high cortisol weakens you more.




Nishan Basnet
March 20, 2026 AT 12:30Just read this through twice. The way cortisol eats away at your body like acid is terrifying-but also so accurate. I’ve seen patients with buffalo humps so severe they couldn’t lie flat. And the stretch marks? They’re not just skin deep. They’re literal tears in the dermis. Surgery isn’t cosmetic-it’s structural repair. If you’ve got endogenous Cushing’s and a confirmed tumor, don’t wait for the next ‘bad week.’ Do it now.
Allison Priole
March 21, 2026 AT 21:29i just want to say that after reading this i felt like someone finally put words to everything i’ve been too tired to explain. my moon face took 3 years to go away after surgery, and i still get weird fatigue sometimes, but like… i can hug my kid without feeling like my bones are gonna shatter. that’s everything. also the part about cortisol making you eat yourself? yeah. that’s the vibe.
Casey Tenney
March 21, 2026 AT 23:39Stop delaying. This isn’t ‘stress.’ This is your body collapsing. Get surgery or accept that you’re choosing a slow death.
Sandy Wells
March 23, 2026 AT 01:56Interesting article but it reads like a pharmaceutical ad. Where’s the data on long-term quality of life? And why no mention of alternative therapies? The tone feels… rushed. Like someone wants you to sign up for a procedure without considering the full picture.
Bryan Woody
March 23, 2026 AT 15:55Let me break this down for you like you’re five: cortisol is your body’s nuclear reactor on meltdown mode. Drugs? They’re like throwing ice cubes at a volcano. Surgery? That’s the damn control rod. And if your surgeon does less than 20 of these a year? You’re basically playing Russian roulette with your pituitary gland. Volume isn’t a buzzword-it’s your survival metric. Also, that FDA device that tells you if the tumor’s gone in 24 hours? Mind blown. Why isn’t this everywhere yet?
Chris Dwyer
March 24, 2026 AT 01:44You’re not broken. You’re just flooded. And surgery isn’t punishment-it’s a reset button. I know it sounds scary, but think of it like rebooting your body’s OS. The fatigue? The moon face? The stretch marks? They’re bugs in the system. Remove the source, and your body knows how to heal. It’s already built-in. You just gotta give it the chance. One step at a time. You got this.
Timothy Olcott
March 25, 2026 AT 23:59Why are we letting big pharma control this? 😒 Surgery is cheaper than lifelong meds but they don’t make money off it. Also, if you're in the US and your insurance won't cover the right surgeon? That's corruption. 💥
Desiree LaPointe
March 27, 2026 AT 07:12How quaint. A 12-page manifesto on cortisol as if it were some divine revelation. Of course, the real issue is that Western medicine has turned hormone regulation into a surgical spectacle. We’ve forgotten that cortisol isn’t a villain-it’s a messenger. Maybe we should be asking why the body is producing so much of it in the first place? Trauma? Environmental toxins? The soul’s silent scream? No. We just cut it out. How… primitive.
Jackie Tucker
March 27, 2026 AT 20:31Of course the article doesn’t mention that 40% of pituitary tumors recur within 10 years. And the ‘success rate’ is inflated because they only count patients who survive the first year. And what about the psychological trauma of being a walking cortisol experiment for years? No one talks about that. The real cure? Leaving the system. But that’s too inconvenient for a medical blog, isn’t it?
Nicole James
March 29, 2026 AT 06:19Did you know cortisol overload is linked to 5G radiation? The towers are designed to trigger adrenal overdrive… and the FDA? They’re in on it. Also, the ‘tumor’ isn’t real-it’s a misdiagnosed biofilm from vaccines. I had mine reversed with magnesium oil and chanting at the full moon. Surgery? No thanks. I’m not a lab rat.
Shaun Wakashige
March 29, 2026 AT 14:02cool article i guess. i just like how it says surgery is the answer but doesn't say anything about how hard it is to find a good surgeon. like, where do i even go? 😐
Paul Cuccurullo
March 30, 2026 AT 12:28Thank you for this comprehensive overview. It is clear that surgical intervention remains the most effective means of restoring homeostasis in endogenous Cushing’s Syndrome. The data supporting volume-outcome correlations is compelling and warrants greater institutional prioritization. I would only suggest expanding the discussion on postoperative psychological rehabilitation, as emotional recovery often lags behind physiological improvement.
Solomon Kindie
March 31, 2026 AT 12:24So you're saying if you're rich and live near a big city you get fixed but if you're poor and in flyover country you just get a pill and told to chill? And the fact that the article doesn't even mention the fact that women are misdiagnosed 3x more often because doctors think it's just 'stress' or 'menopause' is wild. This whole thing is a class issue wrapped in medical jargon. Also, typo: 'adrenalin' should be 'adrenal'.