Imagine your kidneys as a high-tech water filtration system for your body. At the heart of this system are millions of tiny clusters called glomeruli. Their job is simple but vital: keep the good stuff (like proteins and blood cells) in your veins and flush the waste out through your urine. But what happens when your own immune system, designed to fight off viruses, suddenly decides these filters are the enemy? That is exactly what happens with Glomerulonephritis is a group of immune-mediated kidney disorders where inflammation damages the glomeruli, compromising the blood-filtering process.
When these filters get inflamed, they leak. Instead of a clean filtration process, proteins and red blood cells slip through into the urine. For some, this happens suddenly after a throat infection; for others, it is a slow burn caused by a chronic autoimmune disease. Either way, if left unchecked, it can lead to permanent kidney scarring and failure. Understanding how this happens is the first step in managing the condition and protecting your renal health.
The Anatomy of a Filter Failure
To understand how the damage happens, you have to look at the glomerular filtration barrier. Think of it as a three-layered sieve. First, there is the endothelial glycocalyx and the endothelial cells, which act as the initial screen. Then comes the glomerular basement membrane (GBM), a tough structural layer. Finally, there are the podocytes, which are specialized cells that wrap around the capillaries like fingers to create final, precise slits for filtration.
In a healthy kidney, these layers work in perfect harmony. However, in glomerulonephritis, the immune system attacks these structures. Podocytes are particularly vulnerable because they can't easily regenerate. Once an immune attack destroys a podocyte, the "hole" in the filter stays open, leading to massive protein loss. This isn't just a technical failure; it's a systemic problem. When proteins leak out, the blood loses its ability to hold onto water, which is why many patients wake up with swollen ankles or puffy eyes.
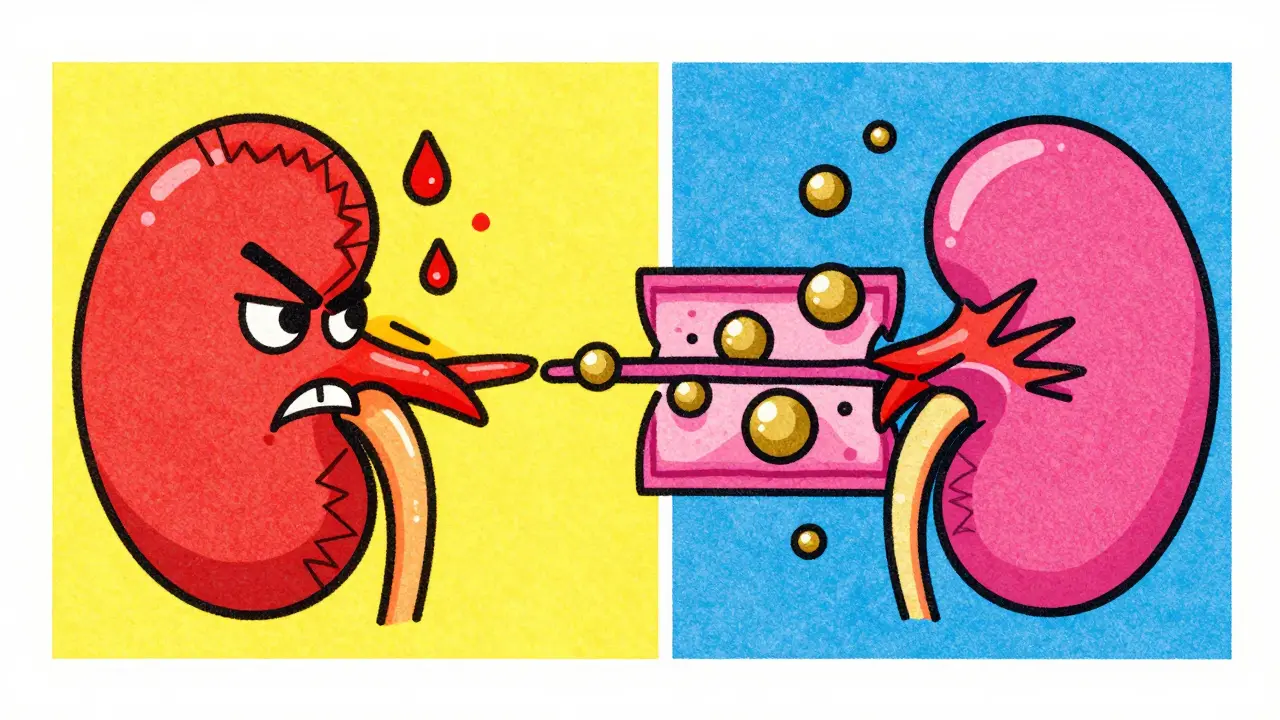
Spotting the Signs: Nephritic vs. Nephrotic
Not all kidney filter attacks look the same. Doctors generally group the symptoms into two main "syndromes." Knowing the difference helps in figuring out which part of the immune system is causing the chaos.
Nephritic Syndrome is characterized by an "angry," inflamed filter. You'll often see blood in the urine (hematuria) and a sudden spike in blood pressure. This happens because the inflamed filters can't clear water and salt effectively, causing fluid to build up in the bloodstream. You might see serum creatinine levels climb to 1.5-3.0 mg/dL, signaling that the kidneys are struggling to keep up with the workload.
Nephrotic Syndrome is more about "leakiness." The inflammation might be less aggressive, but the barrier is compromised. The hallmark here is massive proteinuria-leaking more than 3.5g of protein per day. This leads to hypoalbuminemia (low blood protein) and hyperlipidemia, where LDL cholesterol often climbs above 160 mg/dL. The result is severe edema, where fluid leaks from the blood vessels into the surrounding tissues, making the skin feel tight and swollen.
| Feature | Nephritic Syndrome | Nephrotic Syndrome |
|---|---|---|
| Primary Symptom | Blood in urine (Hematuria) | Protein in urine (Proteinuria) |
| Blood Pressure | Often high (Hypertension) | Usually normal |
| Fluid Retention | Mild to moderate edema | Severe, generalized edema |
| Blood Chemistry | Elevated Creatinine | Low Albumin / High LDL |
The Different Faces of the Disease
Because the immune system is complex, it can attack the filters in several different ways. Some of these are "primary," meaning the disease starts in the kidney. Others are "secondary," meaning the kidney is just a victim of a larger body-wide problem.
- IgA Nephropathy: This is the most common primary form globally. It happens when an antibody called IgA builds up in the kidney tissue. In North America, it affects about 2.5 per 100,000 people yearly, and unfortunately, 20-40% of these cases can progress to end-stage renal disease over two decades.
- Lupus Nephritis: A secondary form where Systemic Lupus Erythematosus (SLE) causes the body to attack its own tissues. About 50-60% of people with lupus develop this kidney complication.
- C3 Glomerulonephritis (C3G): A rarer, more aggressive form involving the complement system-a part of the immune system that "complements" the ability of antibodies to clear pathogens. In C3G, the complement protein C3 goes haywire, accumulating in the filters at levels 3-5 times higher than normal.
- Post-Streptococcal GN: Often seen in children after a strep throat infection. The good news? About 95% of these children recover fully within two months.
How Doctors Unmask the Attack
You can't diagnose the exact type of glomerulonephritis with a simple blood test or a urine dipstick. While those tests show that something is wrong, they don't show what is wrong. To get a definitive answer, a nephrologist usually performs a kidney biopsy.
A biopsy involves taking a tiny piece of kidney tissue to examine it under a high-powered microscope. Pathologists look for specific patterns, such as "electron-dense deposits" (clumps of immune complexes) which are found in 95% of cases of Membranoproliferative Glomerulonephritis (MPGN). This process isn't without risk-about 3-5% of patients experience complications like bleeding. It also requires a high level of expertise; nephropathologists typically need 5-7 years of specialized training to tell these subtypes apart accurately.
Managing the Fire: Treatment Realities
Once the type of attack is identified, the goal is to stop the immune system from destroying more filters. For decades, corticosteroids (like prednisone) have been the first line of defense. They act like a fire extinguisher, dousing the inflammation throughout the body.
But these drugs come with a heavy price. A study by NEPTUNE found that 30-50% of patients experience significant failures or severe side effects. Many struggle with rapid weight gain, increased infection risks, and a terrifying loss of bone density. One patient reported developing severe osteoporosis and two vertebral fractures within just 18 months of prednisone use. It's a difficult trade-off: save the kidneys, but risk the bones.
The tide is turning toward "targeted therapies." Instead of shutting down the entire immune system, new drugs target specific pathways. For example, eculizumab is used for C3G to block the overactive complement system, reducing protein leakage by 40-50% in a year. However, these breakthrough drugs are incredibly expensive, sometimes costing $500,000 annually, which creates a massive gap in care between wealthy and low-income regions.

Living with the "Silent" Struggle
For those living with GN, the physical symptoms are only half the battle. Fatigue is a crushing reality, with 65% of patients reporting it as a major hurdle. Managing edema-the swelling in the legs and face-is a daily struggle mentioned in nearly 80% of patient forum discussions. There is also the mental toll; the anxiety of wondering if you will eventually need dialysis is a constant companion for many.
The journey to diagnosis can also be frustratingly slow. Some patients report spending over four months and seeing three or more specialists before getting a clear answer. The lesson here is clear: if you notice persistent foam in your urine (a sign of protein) or blood-tinged urine, don't wait. Early intervention, such as starting targeted medications like rituximab shortly after diagnosis, can be the difference between maintaining kidney function and needing a transplant.
What causes glomerulonephritis?
It is caused by an immune system malfunction. This can be a primary attack where the immune system targets the kidney filters directly (like in IgA nephropathy) or a secondary attack resulting from a systemic disease like lupus or a previous infection like strep throat.
Can glomerulonephritis be cured?
Whether it can be "cured" depends on the type. Post-streptococcal GN in children often resolves completely. However, chronic forms like IgA nephropathy or lupus nephritis are typically managed rather than cured, with the goal of slowing progression to kidney failure.
Why is a kidney biopsy necessary?
Blood and urine tests can show that the kidneys are failing, but they can't show the exact pattern of damage. A biopsy allows pathologists to see the actual structure of the glomeruli and identify specific immune deposits, which is the only way to choose the correct targeted treatment.
What are the main side effects of steroids used for GN?
Common side effects include significant weight gain, mood swings, increased susceptibility to infections, and a decrease in bone density (osteoporosis), which can lead to fractures.
What is the difference between proteinuria and hematuria?
Proteinuria is the presence of excess protein in the urine, which makes the urine look foamy and often leads to swelling (edema). Hematuria is the presence of red blood cells in the urine, which can make the urine look pink, red, or cola-colored.
Next Steps and Troubleshooting
If you are managing a diagnosis of glomerulonephritis, your priority should be a strict monitoring schedule. Most guidelines suggest checking serum creatinine every two weeks in the early stages and monitoring proteinuria monthly. Keep a detailed log of your weight and any new swelling, as these are early warning signs that your current medication may need adjustment.
For those struggling with steroid side effects, talk to your doctor about "steroid-sparing agents." These are medications that allow you to lower your prednisone dose while still keeping the inflammation under control. If you are in a region with limited access to the newest targeted therapies, seek out university-affiliated research hospitals, as they often have access to clinical trials for drugs like iptacopan that aren't yet available in general practice.




Nikita Shabanov
April 27, 2026 AT 06:04It is important to mention that while monitoring creatinine is vital, patients should also keep a close eye on their blood pressure readings at home. High blood pressure can both be a symptom and a cause of further glomerular damage, creating a vicious cycle that accelerates kidney failure.
Edwin Perez
April 27, 2026 AT 22:33Funny how these "targeted therapies" suddenly cost half a million dollars. Follow the money and you will see it is just a way for Big Pharma to keep us dependent on overpriced chemicals while they hide the real causes of immune dysfunction.
Anand Mehra
April 29, 2026 AT 03:29medical science just a game of trial and error. calling it a guide is a stretch when most of this is just guessing until the biopsy hits
Daniel Runion
April 30, 2026 AT 08:12Wait, why are we pretending that steroids are the only option??? Everyone knows that diet and holistic inflammation control are just as effective, if not more so, than those bone-melting drugs!!! The medical establishment loves to ignore the basics because there is no profit in eating clean!!!
Hayley Redemption
May 1, 2026 AT 06:25The simplistic dichotomy between nephritic and nephrotic syndromes presented here is almost quaint. In actual clinical practice, the overlap is far more nuanced, and pretending they are distinct buckets is a hallmark of amateur medical writing.
William Zhigaylo
May 2, 2026 AT 08:07Your blatant disregard for the precision of these diagnostic tools is utterly repulsive. A biopsy is the gold standard for a reason, and to suggest otherwise is not only ignorant but dangerous to anyone actually suffering from these pathologies.
Brittney Prince
May 3, 2026 AT 20:38Exactly. Biopsies are just another way for them to get more tissue samples for their secret labs. Don't trust the needles.
Sharyl Foster
May 4, 2026 AT 17:18Actually, the biopsy risk is totally blown out of proportion. I've seen plenty of people get them with zero issues. Also, the "silent struggle" part is just melodrama; it's a chronic illness, people deal with it.
Vijay AGarwal
May 4, 2026 AT 20:00Listen, the pain of edema is absolutely soul-crushing! Imagine waking up and your eyelids are so swollen you can barely open them to see the world! It is a nightmare that no one talks about enough! People need to understand the sheer agony of feeling your own skin stretch to the breaking point while your energy vanishes into thin air! It is an invisible prison that steals your youth and your spirit!
sachin singh
May 6, 2026 AT 19:43It is truly heartening to see the progress in targeted therapies like eculizumab.